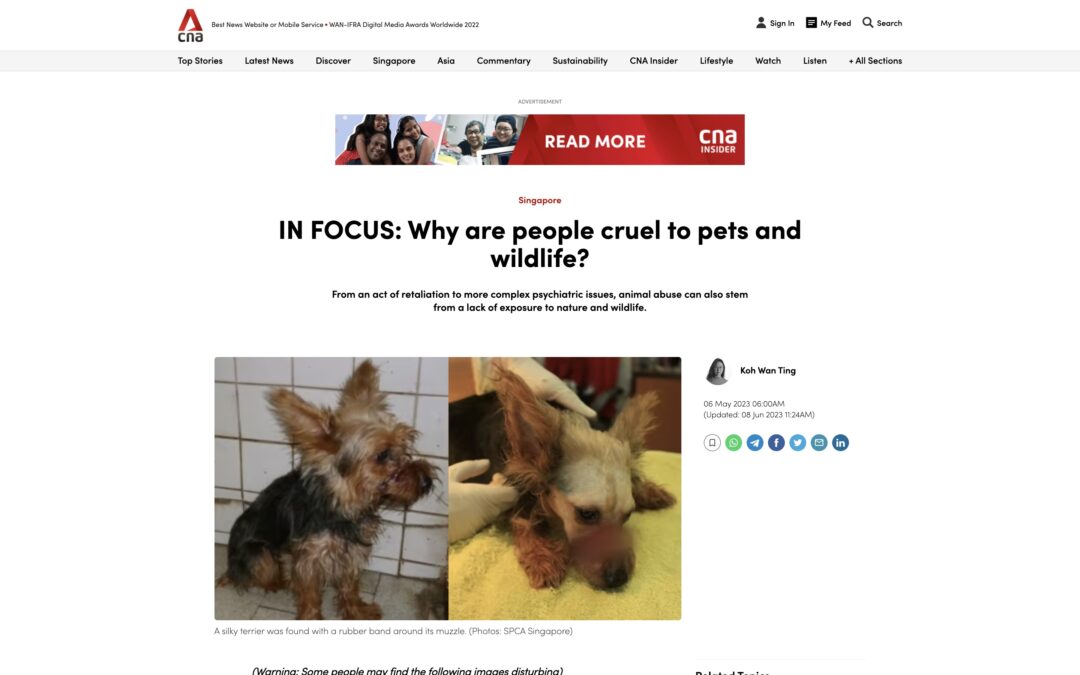
In this CNA article written by Koh Wan Ting, she shares that in recent years, the Society for the Prevention of Cruelty to Animals (SPCA) and other animal welfare groups have witnessed a disturbing rise in cases of animal abuse. From heart-wrenching instances of pets subjected to extreme cruelty to wildlife suffering at the hands of fearful humans, the reasons behind such acts are both varied and complex. In a candid discussion with mental health professionals, animal welfare organizations, and authorities, the motivations behind these acts of cruelty are brought to light. Dr. Rajesh Jacob, a distinguished senior consultant psychiatrist at Promises Healthcare, shares his insights into the possible underlying mental health issues contributing to this disturbing trend.
Understanding the Motivations: Cruelty towards animals can arise from several factors. While some cases involve acts of retaliation or ignorance about proper animal care, more complex psychiatric issues can also drive abusive behavior. Dr. Jacob points out that individuals with conditions like antisocial personality disorder often lack empathy and derive pleasure from seeing others suffer, making them prone to violence, including animal abuse.
The Role of Exposure and Education: The lack of exposure to nature and wildlife can play a significant role in fostering intolerance towards animals perceived as dangerous. As humans become more disconnected from nature and encounter wildlife in unexpected places, fear may lead to harmful actions, as seen in the tragic case of a paradise tree snake killed with boiling water in a preschool. Animal Concerns Research and Education Society (ACRES) co-CEO, Anbarasi Boopal, emphasizes the need for increased awareness and education to dispel misconceptions and promote coexistence with wildlife.
The Disturbing Trend Among Youth: A concerning trend involves youth and children involved in intentional acts of animal cruelty. Dr. Jacob highlights the novelty element, where children may replicate harmful actions seen on social media for fun or amusement. Moreover, children from dysfunctional families or with conduct disorders may engage in abusive behavior due to a lack of empathy and the normalization of violence. Early intervention through therapy and education is crucial in curbing such tendencies.
Addressing the Problem and Seeking Justice: In investigating animal cruelty cases, authorities like the Animal and Veterinary Service (AVS) play a vital role. However, lack of evidence, the emotional cremation of abused animals, and the absence of eyewitnesses can hinder the process of seeking justice. Experts and animal welfare organizations call for stricter penalties for animal abusers and measures to prevent them from owning pets in the future.
The growing incidence of animal cruelty calls for a multi-pronged approach, combining mental health intervention, education, and stricter penalties. By fostering empathy and promoting responsible pet ownership from a young age, we can work towards building a more compassionate society where animals are treated with care and respect. Dr. Rajesh Jacob and other experts emphasize the importance of understanding the root causes behind such acts, enabling us to take proactive steps to prevent and address animal cruelty effectively.
CNN Digital spoke with Dr Jacob Rajesh to give his views regarding a case that shocked the nation of Japan where a teenage girl was stabbed to death by her elderly grandfather.
Here’s his quote:
Jacob Rajesh, a senior forensic psychiatrist at the Promises Healthcare facility in Singapore, said in cases of rapidly progressing Alzheimer’s “it will be difficult to provide an accurate account of what actually happened.”
“There is also the question of fitness to stand trial – is a person fit enough to give evidence on the stand and plead guilty or not guilty?” he said.
Crimes involving dementia patients are also extremely complex, experts said.
In these trying times, mental health is on many people’s minds! While therapy in Singapore has become more accepted, some people still feel trepidation when it comes to psychiatric medication for depression and antidepressants. They also want to know more about side effects and new treatments like Transcranial Magnetic Stimulation (TMS). DR JACOB RAJESH from Promises Healthcare shares his view on all of these things.
What are some commonly used psychiatric medications?
Depression is a very common disorder, affecting between five to ten percent of people, so we use antidepressants quite often. The medications we’ve been using for the past 25 years are called Selective Serotonin Reuptake Inhibitors (SSRIs). These newer generation drugs have much fewer side effects than those used in the past.
They do have some side effects though, the most common being gastric distress, nausea, headaches and insomnia. Some people also report sexual dysfunction and decreased libido. However, these side effects can be managed once the medication and dose is adjusted. SSRIs are usually more tolerated than older antidepressants.
Another group of drugs is the antipsychotics, which are used to treat schizophrenia and bipolar disorders. The second generation antipsychotics have fewer side effects than older ones, along with fewer cognitive effects and extrapyramidal side effects such as causing tremors or stiffness. However, side effects such as weight gain, increased blood sugar and increased cholesterol can occur with some of these drugs; these side effects need to be screened for on a regular basis
Is psychiatric medication an alternative to therapy? Or do they work hand in hand?
Medication and therapy usually work hand in hand. Being medication-compliant is another important part of the mental health recovery treatment as it helps bring stabilisation to the chemical and biological changes in the sufferer that cause the disorder.
For depression, we prescribe medication for moderate or severe symptoms if it’s causing impairment or distress. We also recommend psychotherapy in its various forms: cognitive behavioural therapy, dialectical behaviour therapy, acceptance and commitment therapy, interpersonal therapy or family therapy, depending on the psychosocial stressors.
For bipolar disorder or psychotic conditions like schizophrenia, medications are the mainstays of treatment. However, psychotherapy methods can also help with regulating emotions and give handles to help regulate distorted thoughts when mild symptoms occur. Psychological therapy also plays a role for Obsessive-Compulsive Disorder (OCD) and eating disorders. Here, psychotherapy has a much more important role.
What are some of the misconceptions people have about psychiatric medication?
The most common misconception is that all psychiatric medications make you feel like a zombie – you can’t function, you can’t go to work, your mental faculties are affected. While some of the older generation antipsychotic medications can cause mental fogginess, there are newer ones with fewer side effects. Some people also believe that if they start taking medication, they might become addicted. It is usually the benzodiazepine class of drugs that are addictive in the long term; antidepressants aren’t addictive in the long term. We also see many patients who’ve been taking medication on a long-term basis, but we work with them to minimise side effects. We do this by adjusting the dosage, changing the class of drugs used and lifestyle modification. It’s also worth mentioning that psychologists cannot prescribe any of these drugs, only psychiatrists can.
Can you tell us more about new techniques like Transcranial Magnetic Stimulation?
Transcranial Magnetic Stimulation (TMS) uses electromagnetic waves to stimulate the brain. Unlike electroconvulsive therapy, which is more for people with severe psychotic depression, TMS doesn’t require any sedation. The patient simply sits in a chair and has a device placed at specific parts of the brain where it sends small electromagnetic waves. It is an outpatient procedure and there aren’t usually any side effects.
TMS is used primarily for people with depression who haven’t responded to antidepressants or have severe side effects from medication. It’s not usually a first-line procedure.
Is it as effective as antidepressants?
It works in combination with them. If that alone isn’t helping, TMS can augment the medication. It can also help by itself, but once the treatment stops the patient can relapse, so it’s better to take medication along with it.
What are some psychiatric issues that people may not realise they have?
Many people don’t realise that depression or anxiety disorders are mental illnesses. They think it’s a weakness in their own personality or the result of external stressors they can’t handle. The stigma of mental disorders also plays a big part. People tend to be quick to seek help for physical issues but still feel uncomfortable seeing a psychiatrist. I think it’s becoming more accepted though. There’s a misconception that psychiatrists just provide medication.
What else do they do?
Psychiatrists work in teams. The team-based approach is very important because we have psychiatrists who are qualified doctors along with psychologists who are trained in psychotherapy. We also have social workers, case managers and occupational therapists.
It’s a misconception that psychiatrists cannot do therapy. There are many psychiatrists who are trained in many forms of therapy, but the psychologists are the professionals who study these critical areas in depth. We refer the patients to them because it is their area of expertise.
What would you tell someone who is unsure about seeking help?
Don’t be ashamed of your symptoms or be self-critical. Many feel their symptoms stem from a weak personality or an inability to handle stress. People need to understand that mental health issues can occur for people who’ve done everything right – people with a good job, a good family life, good support and no financial issues. Depression is a biological response and it can happen without any external stressors so there is no shame in seeking help.
Dr Rajesh is a Senior Consultant Psychiatrist at Promises Healthcare, a provider that offers a wide range of psychiatric and psychological services for patients of all ages. Promises is also the only private centre in Singapore to offer Transcranial Magnetic Stimulation.
For more information on psychiatric medication and treatments offered by Promises Healthcare, click here. #09-22/23 Novena Medical Center | 6397 7309
Dinesh is a seasoned writer and editor with seven years of experience covering travel, restaurants and bars. His interests include film photography, cheesy 90s monster flicks, and scouring the island for under-the-radar craft beer bars.
The discussion touched on a wide range of Mental Health conditions that they are concerned over; explained what they are and how one could cope or be a support.
We encourage you to hit the ‘play’ button to view the video.
So if you feel anxious, depressed, stressed, or even suicidal? What can you do? Too many people suffer in silence and don’t seek help! Come join a conversation about mental health issues! Our experienced panel will consist of mental health professionals from various disciplines, a Senior Consultant Psychiatrist, Senior Clinical Psychologist from Promises Healthcare Clinic, and an Assistant Head of a Family Service Centre! The panel will be moderated by Casework Manager of SG Accident Help Jevon Ng, an advocate for mental health and wellbeing. Our panel members all have a lived experience of mental health and will be answering questions from the audience.audience participation is encouraged. Please click the link below to join the webinar: https://us02web.zoom.us/j/83397902082Date: Saturday, May 16 2020Time: 4:30 pm – 6:30 pmEvent Categories: Raise Awareness Organizer@Migrant workers Singapore Support by SGcare Physiotherapy Clinic
The basic characteristics of all religions are similar. There is a firm belief in a higher unseen power who is the supreme master.
Religion and Spirituality, Is There A Difference?
Religion Is an organized system of beliefs, practices, rituals, and symbols designed to facilitate closeness to the sacred or transcendent (God, higher power, or ultimate truth/reality).
Spirituality is the personal quest for understanding answers to the ultimate questions about life, about meaning, and about the relationship with the sacred or transcendent, which may (or may not) lead to or arise from the development of religious rituals and the formation of a community. Spirituality is thus a more inclusive concept than religion.
Mental Illness In The Middle Ages
The idea that religion and psychiatry have always been in conflict is still very prevalent. Today, most people believe that in the medieval ages, most mental disorders were considered as witchcraft or demonic possession. People with mental disorders were recognized as different and treated in various ways. Early medicine men, considering such individuals to be possessed by demons, introduced a technique called trephination, which Involved drilling a hole in the head of the individual to let evil spirits out of the body. Many other civilizations independently developed such a procedure. For example, among the remains of the Incas in Peru are skulls with holes and trephination devices. The treatment of mental illness deteriorated in the late Middle Ages and remained poor through the eighteenth century. As the medieval years progressed, insanity became linked to witchcraft and demon possession. Those considered to be possessed with demons were exorcised. This ritual, performed by a priest, would call upon the demon to come out of the individual and to transfer itself into an animal or inanimate object. Both the Greeks and Romans thought that the mentally ill were capable of causing major social problems, as well as harm to themselves. They made provisions for guardians to take care of the insane. Realizing that these people could hurt themselves or others and could destroy life and property, laws were passed that set specific guidelines. Since there were no lunatic asylums, people with mental illness were a family responsibility. The seriously impaired were restrained at home, but others were permitted to wander in the hope that evil spirits might fly out of them.
Certain saints were thought to be more active in the domain of madness. In northern France, the shrines of Saint Mathurin at Larchant and Saint Acairus at Haspres were known for healing. In Flanders, now Belgium, citizens of Geel developed a shrine to Saint Dymphna that became a hospice to house the mentally ill. During the early years of the Middle Ages, the community took care of the mentally ill. Later, hospices, then asylums were developed to house them. London’s Bethlem asylum—better known as Bedlam—was founded in 1247, making it one of the oldest institutions of its kind. The term “bedlam” became associated with chaos, confusion, and poor treatment, which reflected the general attitude toward mental illness at the time. It was only in the nineteenth century that scientists and society began to reconsider deviant behaviour from the perspective of mental illness rather than as a manifestation of evil spirits.
Religion And Psychiatry
Persons with mental disorders can sometimes present with symptoms such as hyper-religiosity (manic episodes as part of bipolar disorder) or delusional beliefs such as possessing godly or religious powers. Rates of religious delusions in schizophrenia remain high. These symptoms and signs need to be carefully assessed by mental health professionals. Certain groups in Christianity such as Pentecostal Christians “speak in tongues”, which is not a symptom of mental illness, but an expression of their religious beliefs. “Speaking in tongues” is mentioned in the Bible.
In the last two decades, rigorous scientific research has been done and published in mainstream medical and psychological journals. David B. Larson, Jeffrey S. Levin and Harold G. Koenig were some of the authors. They have conducted a series of studies looking at the relationship between religious involvement and mental health in mature adults, either living in the community or hospitalized with medical illness. Since then, many other researchers have produced a large body of research that has usually, but not always, shown a positive association between religious involvement and mental health.
According to the Harvard psychologist, Gordon Allport, a person’s religious orientation may be intrinsic and/or extrinsic.
Extrinsic Orientation Persons with this orientation are disposed to use religion for their own ends. Many find religion useful in a variety of ways – to provide security and solace, sociability and distraction, status and self-justification.
Intrinsic Orientation Persons with this orientation find their master motive in religion.
Other needs, strong as they may be, are regarded as of less ultimate significance, and they are, so far as possible, brought in harmony with the religious beliefs. Having embraced a creed, the individual endeavours to internalize it and follow it fully. Usually, the intrinsic orientation is associated with healthier personality and mental status, while the extrinsic orientation is associated with the opposite. Extrinsic religiosity is associated with dogmatism, prejudice, fear of death, and anxiety, it “does a good job of measuring the sort of religion that gives religion a bad name.
Physical health: Religiousness was related to decreased smoking and alcohol consumption. Religious commitment and participation seemed to affect longevity, as well, especially in men.
Suicide rates were consistently found to have a negative correlation with religiosity. In Hinduism, if you take your life prematurely, you have to suffer in the next birth. Most research findings support that religious affiliation, especially participation, lowers the rate of alcohol consumption. Being religious results in more hope and optimism and life satisfaction.
Belief Systems, Cognitive Framework
Beliefs and cognitive processes influence how people deal with stress, suffering and life issues.
Religious beliefs can provide support through the following ways: Enhancing acceptance, endurance, and resilience. They generate peace, self-confidence, purpose, forgiveness to the individual’s own failures, and positive self-image. On the other hand, they can sometimes bring guilt, doubts, anxiety and depression through an enhanced self-criticism. ‘Locus of control’ is an expression that arises from the social learning theory and tries to understand why people react in different ways even when facing the same problem. An internal ‘locus of control’ is usually associated with well-being and an external one with depression and anxiety. A religious belief can favour an internal ‘locus of control’ with an impact on mental health.
Religious practices
Public and private religious practices can help to maintain mental health and prevent mental diseases. They help to cope with anxiety, fears, frustration, anger, anomie, inferiority feelings, despondency and isolation. The most commonly studied religious practice is meditation.
It has been reported that it can produce changes in personality, reduce tension and anxiety, diminish self-blame, stabilize emotional ups and downs, and improve self-knowledge. Improvement in panic attacks, generalized anxiety disorder, depression, insomnia, drug use, stress, chronic pain and other health problems have been reported. Follow-up studies have documented the effectiveness of these techniques.
Role of the Psychiatrist
During assessment, the psychiatrist should be able to determine whether the religion in the life of his patient is important, has a special meaning and is active or inactive. Four basic areas should be remembered when taking a spiritual history.
Does the patient use religion or spirituality to help cope with illness or is it a source of stress, and how?
Is the patient a member of a supportive spiritual community?
Does the patient have any troubling spiritual question or concerns?
Does the patient have any spiritual beliefs that might influence medical care?
The clinician who truly wishes to consider the bio-psycho-social aspects of a patient needs to assess, understand, and respect his/her religious beliefs, like any other psychosocial dimension.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok